









AltiVate Reverse®
Category: DJO Shoulder
Reaching Higher by Design
The anatomically-based, data-driven AltiVate Reverse system incorporates enhanced fixation technologies and precision instrumentation for superior fit in more patients.
![]() Proven Results
Proven Results
Elevating the 10-year clinical success of the RSP®, the first reverse shoulder design to successfully incorporate a center of rotation (COR) lateral to the glenoid, DJO Surgical introduces its latest Extremity Solution. The AltiVate Reverse system incorporates an optimized stem design based on anatomic studies with CT scans for determination of shell-to-stem position as well as the ability to best match patient anatomy for anatomic total and reverse total shoulder constructs. The enhanced fixation technologies and precision instrumentation ensure the AltiVate Reverse stem will have a superior fit in more of your patients.

FEATURES & BENEFITS

ANATOMIC BASIS

The AltiVate Reverse stem was designed using anatomic studies to optimize the shell-to-stem position and to match patient anatomy for both anatomic and reverse total shoulders. This stem features an anatomic humeral neck-shaft angle of 135°.
Biomechanical testing has shown that having a humeral neck-shaft angle in the range of normal anatomy reduces the potential for inferior scapular notching.1
ENHANCED FIXATION
 On both the glenoid and humeral side, expect short and long term fixation as a result of stable initial fixation as well as ideal conditions for bony ingrowth.
On both the glenoid and humeral side, expect short and long term fixation as a result of stable initial fixation as well as ideal conditions for bony ingrowth.
Our one piece, monolithic AltiVate Reverse glenoid baseplate design provides 2000N or 10X more compression than a pegged baseplate design,3 providing stable initial fixation. The coating options, P2 and 3D Matrix with hydroxyapatite, create ideal conditions for bony ingrowth for long-term fixation.
P2, backed by the largest porous coating animal study in the world, creates instant micro-fractures in the trabeculae upon initial bite to the bone, which causes an instantaneous bone in-growth reaction.2
CLINICAL APPLICATION
The AltiVate Reverse stem is indicated for a variety of applications:
For each of these applications, the stem can be cemented or press-fit.
VERSATILITY FOR COMPLEX ANATOMY
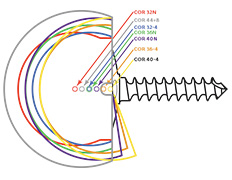
Glenospheres
A great deal of variability can be experienced in rotator-cuff-deficient shoulders. The AltiVate Reverse system offers unmatched versatility, in size and offset, of glenospheres to manage complex anatomy and surgical outcomes

Socket Inserts
Both traditional and +4mm inserts are available in 32, 36, 40 and 44mm in standard and semi-constrained providing various options of height, diameter, and constraint.
![]()
8mm Spacer
This 8mm Spacer is screwed into the AltiVate Reverse Stem and with a traditional insert provides 8mm of humeral prothesis build-up.

Hemi-Adapter
This Hemi-Adapter is screwed into the AltiVate Reverse Stem and with a Turon humeral head converts the reverse stem to a hemi-arthroplasty prosthesis.
PRECISION INSTRUMENTATION
The AltiVate Reverse instrumentation was designed for two different surgical approaches, catering to different surgical preferences. The instruments simplify prosthesis positioning and implantation, and specialized revision instruments allow for stem removal with minimal bony disruption.
Metaphyseal-Referenced
Implant position is based on the fit in the metaphysis.
 |
 |
 |
 |
 |
 |
 |
| Osteotomy | Create centered pilot hole | Protect and move to glenoid | Ream Socket | Ream Canal | Assemble trial shell and broach | Impact trial assembly |
Diaphyseal-Referenced
Implant position is based on the fit in the humeral canal.
|
|
|
 |
|
 |
 |
|
 |
| Osteotomy | Ream Canal | Broach | Protect and move to glenoid | Add reaming / planing guide pin | Plane | Ream Socket | Insert socket trial |
 Loading...
Loading...